J Chron Dis 12;586-591 (Dec) 1960
Epidemiology
Relations between Hardness of Water and Death Rates from
Certain Chronic and Degenerative Diseases in the United
States
Henry A. Schroeder, M.D.
West Brattleboro, Vt.
From the Department of Physiology, Dartmouth Medical
School and the Brattleboro Retreat
(Received for publication April 9, 1960)
Death rates vary widely from state to state. Significant
negative correlations between weighted average hardness of water
supplies and death rates from cardiovascular diseases in the
United States have been reported.1 In States supplied
with harder-than-average water, average annual age-adjusted death
rates from all causes and from cardiovascular diseases for both
sexes, for males, for females, and for white males aged 45 to 64
years, were in general lower than national averages. These
relationships applied to death rates from coronary heart disease
as well as to rates from all other cardiovascular diseases. Rates
for Coronary heart disease in older white males correlated
significantly with hardness and with a number of constituents of
drinking water in the 163 largest municipalities of the country.
Correlations were absent for deaths from all other
causes.1
In order to define these interesting relations further, the
present report examines correlations by state between weighted
average hardness of "finished"* water (an
index of exposure per person) and average annual death rates from
a number of chronic and degenerative diseases for the years 1949
to 1951.2 Correlation coefficients (r values) were
calculated by the usual method.3 Values for water were
measured in 1950 to 1951.4 Diseases listed among the
ten leading causes of death and subdivisions thereof with
relatively high death rates in the decade 55 to 64 years were
chosen in order to avoid, as much as possible, rates possibly
erroneous because of small numbers of cases. This consideration
applied in general to death rates less than 10 per 100,000
persons.
States which have harder water than the national average are
all those in the East North Central (5 states), West North
Central (7 states), and Mountain (8 states) areas, plus Florida,
Kentucky, Oklahoma, Texas, and California.5 Therefore,
25 states have water harder and 23 states and the District of
Columbia have water softer than the national average of 97 parts
per million.
It so happens that many "soft-water" states have large
nonwhite populations. The correlation coefficient of hardness of
water and per cent of the non white population per state was
-0.341, which is significant at the 2 per cent level of
confidence. Therefore, death rates of white persons were analyzed
in order to avoid this influence. In all cases, however,
correlation coefficients were calculated as well for all races
and, in most cases, for all ages; these data are reported when
they appear of interest to the problem.
RESULTS
In Table I are shown the correlation coefficients and their
levels of significance for water hardness by state and death
rates from the ten leading causes of death for all ages, races,
and both sexes. Significant values appear mainly in the
cardiovascular group of diseases, motor vehicle accidents, and
congenital malformations. In Table II, confined to white persons
aged 55 to 64 years, major categories are subdivided into their
constituent parts. In white persons the highest negative
correlations occurred with those disorders commonly believed to
be associated with atherosclerosis and with arterial
hypertension, (hypertension with heart disease, vascular lesions
affecting the central nervous system, general arteriosclerosis,
and arteriosclerotic heart disease, including coronary disease);
correlations were not significant in the case of rheumatic heart
disease, nonrheumatic chronic endocarditis and other myocardial
degeneration, chronic nephritis, or "other diseases of heart"
(Table II).
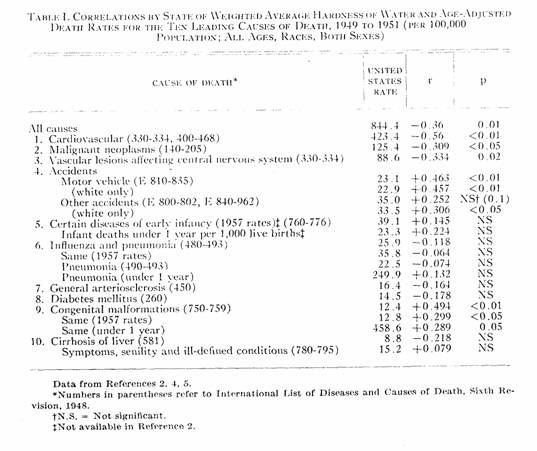
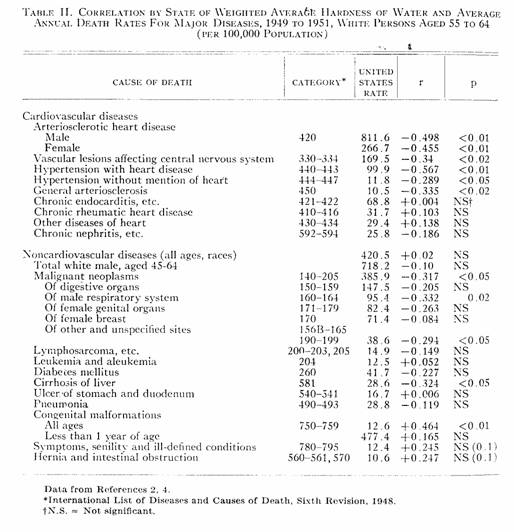
In the case of malignant neoplasms, one probably significant
negative correlation (p = 0.02) appeared for neoplasms of the
respiratory tract in males aged 55 to 64 years. In this decade
there was some relationship (p < 0.05) between water hardness
and death rates from all neoplastic diseases and from those of
unspecified sites; for other carcinomas, lymphomas, and
leukemias, there were no correlations of significance.
Only in the decade 55 to 64 did a possibly significant
negative correlation (p < 0.05) appear for cirrhosis of the
liver. In the case of motor vehicle accident deaths a high
positive correlation was found; for other accidental deaths it
was also positive but not as significant (Table I). The
correlation for congenital malformations, at all ages, was also
positive (p < 0.01). Correlation coefficients were small in
the cases of other major causes of death, e.g., "certain diseases
of early infancy," influenza and pneumonia and total infant
deaths per 1,000 live births (Tables I and II).
DISCUSSION
There seems to be clearly established a relationship between
weighted average hardness of "finished" water and average annual
death rates by states in 1949 to 1951 for diseases associated
with arterial hypertension and disorders secondary to
atherosclerosis. The high correlation coefficients, -0.5 or more
for two of these disorders are significant at probability levels
of about one in one thousand. Therefore, if one grants the
validity of the data, this relationship can be accepted. Lack of
significant correlations between water hardness and three major
categories of heart diseases — chronic rheumatic heart
disease, "nonspecific chronic endocarditis and other myocardial
degeneration" (which undoubtedly includes an unknown number of
cases of arteriosclerotic heart disease), and "other diseases of
heart" — points further to a true relation between water
hardness and atherosclerotic and or hypertensive disorders.
Sauer and Enterline6 recently examined a number of
factors which might affect data on death rates and concluded that
variations from state to state were real and were unaccountable
by the quality or quantity of physicians. They also believe that
population and total death rates are fairly accurate. The present
study is based upon their conclusions and upon chemical and
analytical data on specimens of municipal water collected during
the period when the death rates were calculated (1949-1951).
Errors in annual variations were thus largely avoided.
Among the noncardiovascular diseases, a possibly significant
correlation with malignant neoplasms appeared only in respect to
male respiratory tract neoplasia Analyses of less common
neoplasms included in the total were not made, for the death
rates were based on too few cases for valid analyses. A
suggestive relationship appeared for cirrhosis of the liver but
for no other common diseases.
Of the ten leading causes of death, correlations were not
statistically significant for diabetes mellitus, infant deaths,
diseases of early infancy, or pneumonia and influenza, either for
total population or older white persons, with the use of the
rates available for 1949 to 1951 or for 1957. Curiously enough, a
significant positive correlation did appear for congenital
malformations in the total population and in white persons of all
ages, which could not be explored further because of the low
rates in adults. Rates for other diseases were too low in many
states for accurate computation.
The curious positive correlation between water hardness and
motor vehicle accident deaths may be a geographical accident. The
hard water areas are in general those midwestern and mountain
states with large areas and low densities of population, where
long-distance driving is usual. In many, motor vehicle laws are
less strict than in the more crowded seaboard states; perhaps
this factor accounts for the correlation. In order to explore
this factor, a correlation coefficient was determined on total
cardiovascular deaths in older white males by state and density
of population per square mile: r = + 0.279 (p = 0.05). The
coefficient for hardness of water and density of population was
-0.292 ( < 0.05). These coefficients are much lower than that
for water and cardiovascular death rates (-0.56).
It was impossible to compare death rates of white and nonwhite
persons, since the cases were few in many states and in 17 there
were few nonwhite persons, making computations
invalid.2 In order to include as many disorders as
possible, death rates for persons in the decade below mandatory
retirement age were chosen when the values were considered
sufficiently accurate from a statistical
standpoint.2
To ascertain the effects of the inclusion of deaths in
nonwhite persons and errors therefrom on these correlation
coefficients, calculations were made for all categories of
diseases listed. Comparisons of white and total populations
showed relatively minor changes in r values for most of the
cardiovascular diseases; values became statistically significant
only in the case of chronic nephritis when nonwhites were
included. Those for several but not all malignant neoplasms
became significant, as did those for diabetes mellitus, pneumonia
in persons aged 55-64, and general arteriosclerosis, reflecting
the higher incidences of these disorders in nonwhite persons from
"soft-water" states. Therefore, unless both white as well as
total populations are analyzed, errors due to this factor can
appear if death rates differ in the two racial groups.
Yerushalmy and Palmer7 proposed certain procedures
for evaluating etiological and accessory factors in chronic
diseases based on modifications of Koch's postulates. No
inference as to etiological factors is intended in this report,
and the influences associated with hardness of water are
obviously accessory environmental factors at the most. However,
some of the postulates of these authors are partly satisfied by
this study, and some are not. In discussing this matter, it must
he emphasized that correlation coefficients shown in the tables,
while statistically significant, are usually small. In Tables I
and II there are only four values each greater than 0.45.
Yerushalmy and Palmer list the following points:
"1. The suspected characteristic must he found more frequently
in persons with the disease in question than in persons without.
the disease, or
"2. Persons possessing the characteristic must develop the
disease more frequently than do persons not possessing the
characteristic."7
In so far as death rates in white persons are concerned, an
influence associated with hardness of water is found at
ages 55-64 in the cases of hypertensive heart disease and
coronary heart disease, and at all ages in motor vehicle
accidents and congenital malformations. This is only an
influence, for there were no "persons without the disease" in any
state or city, although there were many perhaps without "the
characteristic."7
The third point of these authors, concerned with testing the
association for validity by investigating the relationship of the
characteristic with other diseases, has been investigated and
little or no relationship can be found as far as this
influence is concerned. Four causes of death stand out:
smaller coefficients of correlation, while still considered
statistically significant, may or may not be of actual
significance coefficient of 0.45 is high in any study with such a
large number of possible variables as this one has.
This report serves to emphasize a relationship of certain
chronic disorders with a variable environmental factor to which
all persons are exposed. There may be a cause-and-effect
relation, i.e., some factor in, or not in, different waters
influences these death rates, or each of the two parameters may
be related to a third. In any event, experimental work along
these lines may he rewarding.
SUMMARY
Further inquiry into the relationship between hardness of
finished potable water by state and death rates from the ten
leading causes of death and subdivisions thereof in white persons
55 to 64 years of age disclosed:
1. A. Negative correlations with hypertensive diseases and with
common conditions secondary to atherosclerosis (p <
0.01).
B. No significant correlations with other diseases of the
heart.
2. A. A possibly significant negative correlation (p = 0.02) with
neoplasms of the male respiratory system.
B. No significant correlations with other common neoplasms.
3. A. A suggestive negative correlation (p < 0.05) with
cirrhosis of the liver.
B. No significant correlations with diabetes mellitus, influenza
and pneumonia, infantile disorders, ulcer of stomach or duodenum,
''senility,'' or intestinal obstruction.
4. Positive correlations with motor vehicle accident deaths (p
< 0.01) and congenital malformations (p < 0.01) in all age
groups.
In hardness or softness of potable water may lie a clue to an
influence affecting death rates from hypertension and
atherosclerosis, and possibly a few other chronic disorders.
REFERENCES
1. Schroeder, H. A. : Relation Between Mortality From
Cardiovascular Disease and Treated Water Supplies, J.A.M.A..
172:1902, 1960.
2. National Office of Vital Statistics. Death Rates for
Selected Causes by Age, Color, and Sex, United States and Each
State, 1949 to 1951. Vital Statistics vol. 49, Special Rep. Nos.
16-27, 30-43, 48, 52, 58-60, 1959.
3. Herdan, G. : Statistics of Therapeutic Trials, Amsterdam,
1955, Elsevier Publishing Company.
4. Lohr, E.W., and Love, S. K.: Industrial Utility of Public
Water Supplies in the United States, 1952: Parts 1 and 2,
Geological Survey, Water-Supply Papers 1299 and 1300, Washington,
D. C., 1954, U. S. Government Printing Office.
5. Statistical Abstract of the United States, ed.
80, U. S. Department of Commerce, Washington,
1959.
6. Sauer, H. I., and Enterline, P. E. : Are Geographic
Variations in Death Rates for Cardiovascular Diseases Real? J.
Chron.. Dis. 10:513. 1959.
7. Yerushalmy, J., and Palmer, C. E. : Methodology of
Investigations of Etiologic Factors in Chronic Diseases, J.
Chron.. Dis. 10:27, 1959.
This work was supported by a grant from Ciba Pharmaceutical
Products, Summit, N. J., and by a grant from the U. S. Public
health Service, Grant H-5076.
*"Finished" water is
water which has been treated in municipal treatment plants by
procedures such as chlorination, filtration, softening,
adjustment of pH, control of algae, removal of iron and
manganese, coagulation, and aeration. As such, it is the water
delivered to the tap. "Raw" water has received no treatment.
This page was first uploaded to The Magnesium Web Site on
September 14, 2002
http://www.mgwater.com/
