Contribution of Hard Water to Calcium and Magnesium Intakes
of Adults1
JEAN H. HANKIN, Dr.P.H.2 SHELDON MARGEN, M.D., and
NAOMI F. GOLDSMITH, Ph.D.3
School of Public Health and Department of Nutritional
Sciences, University of California, Berkeley
1Supported by grants from the Bureau of Chronic
Disease, California State Department of Public Health, and the
Research Committee, Bay Area Heart Association. Received for
publication January 31, 1969.
2Present address: School of Public Health,
University of Hawaii, Honolulu.
3The authors are grateful to Dr. Nemat Borhani,
former Chief, Bureau of Chronic Disease, and to the Bureau of
Sanitary Engineering, California State Department of Public
Health, for their assistance; and to the food and beverage
processors for food composition data concerning their products.
We also appreciate the constructive suggestions from this
JOURNAL'S reviewers.
ASSOCIATIONS BETWEEN hardness of drinking water and mortality
from cardiovascular diseases have been reported for the United
States, Great Britain, and Sweden (1-4). Correlations were
negative and showed lower death rates in areas with hard water
supplies. These associations could be due to: (a) the
concentration of calcium or magnesium, the principal cations
contributing to water hardness; (b) trace elements or other
constituents common to hard water; or (c) spurious factors. If
the relationships were due to calcium or magnesium, we would
expect persons consuming hard water to have significantly higher
calcium and magnesium intakes, possibly higher serum and urinary
levels of these minerals, and lower cardiovascular disease rates
than those drinking soft water.
Before comparing hard and soft water consumers, we conducted a
pilot study among adult volunteers in a hard-water community in
California during December 1967 to learn if water made a
significant contribution to the total calcium and magnesium
intakes. This paper describes our preparatory activities for
analyzing reported food intakes, the data collection and results,
and some implications of the findings.
Preparatory Activities
Although the limitations of food composition tables are known,
standard values are needed for estimating usual dietary intakes
in studies of large groups, A primary problem for our survey was
the dearth of published data on the magnesium content of foods,
Because magnesium has been included in the 1968 revision of the
Recommended Dietary Allowances (5), it seems likely that other
investigators may share our concern.
For this study, we compiled the values for calcium and
magnesium of selected foods from several sources. Official
documents of the United States (6), Great Britain (7), and
Germany (8) were our primary references. Additional resources
were the publicatiions of the California Agricultural Experiment
Station (9) and of private or commercial organizations (10-13).
We also obtained unpublished data from the U.S. Bureau of
Commercial Fisheries and from fifteen manufacturers through
personal correspondence. Table 1 classifies the foods
into broad categories, such as "meat and poultry," "eggs and
dairy products," and so on, and includes mean food intakes, the
range of values, and the references for the published values.
Using atomic absorption methods, we analyzed samples of
carbonated beverages for calcium and magnesium.
We designed a seven-day measured record for obtaining
quantitative estimates on food and water intakes and developed
standard methods for converting the reported data into equivalent
gram weights. We also conducted preliminary experiments on
spaghetti and rice for calculating the changes in weight and
volume in cooking. The results indicated a ratio of 1 part dry to
2 parts water for spaghetti or other pastes and a ratio of 1 part
dry to 2.5 parts water for rice.
Data Collection
We selected the community of Brentwood because its water
supply was reported to have relatively high values of calcium and
magnesium, 8.6 and 3.6 mg. per 100 ml., respectively (14). With
the assistance of the local public health and civic leaders, we
arranged a community meeting to recruit adult volunteers. After
presenting our objectives, we demonstrated methods of measuring
and recording intakes of food and water and then distributed
seven-day booklets, directions for recording food preparation and
intakes, household measuring equipment, and stamped envelopes for
returning the records.
Our standards for acceptability of a record were that the
measurements of all items consumed at home be complete. Some
omissions for restaurant dishes, food purchases, or preparation
methods occurred, in which case we telephoned the participants
for clarification. From the reported data, we calculated the
proportion of water in all beverages and in all home-prepared
cereals, soups, stews, casseroles, and legume dishes.
A frequency tally indicated that canned or frozen vegetables
were more popular than fresh cooked varieties during the study
week. Since we could not quantitate evaporation losses in cooking
or the extent of mineral exchange between the water and fresh
produce, we did not calculate the contributions of local water to
these items. It also was not practical to perform experiments on
fresh vegetable cookery due to large individual variations in
product selections and in cooking times. Another omission
pertained to desserts and bread items. We found that most persons
purchased packaged and bakery products or used commercial mixes.
Because the magnesium values of mixes and several baking
ingredients were unknown, we decided to code all items in these
categories according to the available data of comparable prepared
products.
The daily records showed that home water supplies represented
three main categories: hard city, hard well, and softened or
treated city and well waters. We collected random samples of tap
water from the three categories, performed calcium and magnesium
analyses by atomic absorption methods, and used group means for
calculating the contributions of the particular source of water
to the daily intakes. The State Department of Public Health
provided information on the mineral contents of the water
consumed in other California communities. The individual and
group intakes of calcium and magnesium from food and from all
sources of water and the percentage of the total intakes
contributed by water were calculated. We also classified
participants according to their intakes of hard or soft water at
home and compared the percentage contributions of water to
intakes of calcium and magnesium for the two groups.
Results
The laboratory analyses of water samples are shown in Table
2.
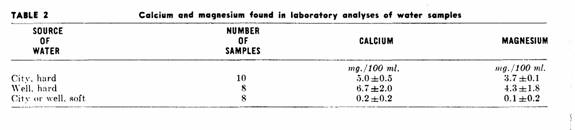
Our data for calcium in hard water were considerably less than
the value of 8.6 mg. per 100 ml reported by the California State
Department o Public Health (14). The difference could be due to
sampling or laboratory methods. We obtained samples from kitchen
taps and used atomic absorption methods, whereas the Department
of Public Health sampled at a central distribution point and used
oxalate precipitation and EDTA or permanganate titration (15).
The analyzed and reported data for magnesium, however, were
similar.
Of the sixty-five adults attending the community meeting,
fifty-six volunteered for the survey. Of these, forty-nine
persons returned the records, while two refused and five did not
respond after follow up phone calls. Four records were rejected
due to incomplete information. The group with acceptable records
included twenty-seven men and eighteen women, representing
thirty-five households. The age of the participants ranged from
twenty-three to seventy-four years.
Water contributed 6.9 ± 5.8 per cent calcium and 12.5
± 9.8 per cent magnesium to the total intakes for the
forty-five participants. Classification of subjects by hard or
soft home water supplies yielded twenty-three in the hard and
twenty in the soft water groups. Two persons consumed both types
of water at home and were omitted from these calculations. For
the two sub-groups, the mean contributions of water for calcium
and magnesium were, respectively: hard water supply, 9.7 ±
6.2 per cent and 18.1 ± 9.2 per cent; soft water supply,
3.4 ±3.2 per cent and 5.4 ± 4.7 per cent.
Discussion
Although these results include the errors of measurement,
interpretation, and food composition, the findings suggest that
food, not water, was the major determinant of the calcium and
magnesium intakes of the forty-five volunteers. We also may
assume that the contribution of hard water to magnesium intakes
was overestimated, because all records included one or more items
of unknown magnesium content. The magnesium values for fresh
meat, poultry, fish, fruits, and vegetables were generally
available, but we found minimal data for items such as cereals,
breads, processed entrées, candies, and desserts. The
diversity and frequency of unknowns made it impractical to select
any particular items for laboratory analyses.
Our compilation of reported food composition values also
revealed large variations for several items. Because we had
little information on the variability of the calcium and
magnesium contents of foods, we were forced to use the means of
the published values. Without knowledge concerning the variation
in these means, the significance of studies such as ours becomes
difficult to interpret. We were pleased that Zook and Lehmann
recently reported both the means and standard deviations in their
analyses of the mineral contents of selected fresh fruits (16).
Their data, published after our study, seem particularly useful,
and we recommend that future publications on food composition
follow similar procedures.
Like other investigators conducting dietary studies in
California (17), we observed large variations in the daily eating
patterns of the Brentwood subjects. The socio-economic status of
these volunteers was probably high, since they were either high
school or college graduates and were engaged in professional,
technical, or business careers. The heterogeneity of their food
habits may be typical of similar groups in a Western society who
volunteer to keep accurate dietary records. Before conducting
this study, we recognized that the frequent use of new food
products and meals eaten in restaurants could increase
measurement and interpretation errors in the food diaries.
Nevertheless, we selected a field study, rather than a metabolic
investigation, to obtain a picture of the usual eating practices
of a larger sample living in a hard water community.
Variation in food patterns and lack of food composition data
were not the only problems in this survey. We found that
residence in a hard water area did not insure an intake of only
hard water. Approximately half of our subjects drank softened or
treated water at home. The participants also were highly mobile,
and several reported drinking water or coffee in six or seven
different localities during the week. This suggests that other
factors, such as the use of home water softeners, place and kind
of employment, and location of restaurants, may be as important
as the reported hardness of the municipal water supply.
Our plans for further research on the relationship of water
constituents and cardiovascular diseases will depend on the
identification of a stable population that consumes primarily
hard, untreated water. We also need additional reliable values
concerning the mineral contents of available food items and hope
that our preliminary survey will stimulate others to perform
laboratory analyses on food composition and on mineral exchanges
in water cookery.
Summary
A pilot study among forty-five adult volunteers living in a
hard-water community of California was conducted to determine the
contribution of water to total calcium and magnesium intakes. A
food composition table was compiled and local water supplies were
analyzed for calculating seven-day calcium and magnesium intakes.
The contribution of water to the total mineral intakes averaged 7
per cent for calcium and 12 per cent for magnesium. The magnesium
contributions were probably overestimated due to lack of nutrient
data for several reported foods.
The frequent use of water softeners and the mobility of the
subjects decreased the expected contributions of hard water to
total calcium and magnesium intakes. Further studies on the
possible relationship of water constituents to cardiovascular
diseases will depend on the identification of a population that
consumes primarily hard, untreated water and on the availability
of additional information concerning the content of foods.
References
(1) SCHROEDER, H. A.: Relation between mortality from
cardiovascular disease and treated water supplies. J.A.M.A. 172:
1902, 1960.
(2) SCHROEDER, H. A.: Municipal drinking water and
cardiovascular death rates. J.A.M.A. 195: 81, 1966.
(3) MORRIS, J. N., CRAWFORD, M. D., AND HEADY, .J. A.:
Hardness of local water-supplies and mortality from
cardiovascular diseases in the county boroughs of England and
Wales. Lancet 1: 860, 1961.
(4) BIORCK G., BOSTROM, H., AND WIDSTROM, A.: On the
relationship between water hardness and death rate in
cardiovascular diseases. Acta. Med. Scand. 178: 239, 1965.
(5) FOOD & NUTR. BD.: Recommended Dietary Allowances,
Seventh Revised Edition, 1968. Natl. Acad. Sci. Pub. 1964,
1968.
(6) WATT, B. K., AND MERRILL, A. L.: Composition of Foods-Raw,
Processed, Prepared. Revised. USDA Agric. Handbook No. 8,
1963.
(7) MCCANCE, R. A., AND WIDDOWSON, E. M.: The Composition of
Foods. 3rd ed. Medical Research Council Special Rept. Series No.
297, 1960.
(8) SOUCI, S. W., FACHMAN, W., AND KRAUT, H.: Die
Zusammensetzung Der Lebensmittel, Nahrwert-Tabellen. Vol. I &
II. (German). Stuttgart: Wissenschaftliche Verlagsgesellschaft
M.B.H., 1962.
(9) HOWARD, F. D., MACGILLIVRAY, J. H., AND YAMAGUCHI, M.:
Nutrient Composition of Fresh California Grown Vegetables. Calif.
Agric. Exper Sta. Bull. No. 788, 1962.
(10) CHURCH, C. F., AND CHURCH, H. N.: Bowes and Church Food
Values of Portions Commonly Used. 10th ed. Philadelphia: J. B.
Lippincott, 1966.
(11) Newer Knowledge of Milk. 3rd ed. Chicago: Natl. Dairy
Council, 1965.
(12) Nutritional Data. 5th ed. Pittsburgh: H. J. Heinz Co.,
1963.
(13) Nutritive Composition of Products. Camden, N. J.:
Campbell Soup Co., 1966.
(14) California Domestic Water Supplies. Berkeley: Bur. of
Sanitary Engin., Calif. Dept. of Pub. Health, 1962.
(15) Personal communication.
(16) ZOOK, E. G., AND LEHMANN, J.: Mineral composition of
fruits. 2. Nitrogen, calcium, magnesium, phosphorus, potassium,
aluminum, boron, copper, iron, manganese, and sodium. J. Am.
Dietet. A. 52: 225, 1968.
(17) HANKIN, J. H., REYNOLDS, W. E., AND MARGEN S. A short
dietary method for epidemiologic studies 2. Variability of
measured nutrient intakes. Amer. J. Clin. Nutr. 20: 935,
1967.
This page was first uploaded to The Magnesium Web Site on
August 28, 2002
http://www.mgwater.com/
